


Click to read
Newsletter
Click to read
June 2012
High-Strength, Metal-Free Alternative to Traditional Denture Prostheses. Innovative techniques provide long-term and patient-pleasing results.
By Stan Lott, CDT, AACD
By Stan Lott, CDT, AACD

Click to read
March 2012
High-Strength, Metal-Free Alternative to Traditional Denture Prostheses. Innovative techniques provide long-term and patient-pleasing results.
By Stan Lott, CDT, AACD
By Stan Lott, CDT, AACD
Click to read
February 2012
The ideal union IPS e.max Press paired with a zirconia framework is the perfect combination for treating edentulous patients.
By Stan Lott, CDT, Accredited Member of the American Academy of Cosmetic Dentistry, AAACD
By Stan Lott, CDT, Accredited Member of the American Academy of Cosmetic Dentistry, AAACD
Click to read
by Precision Elite
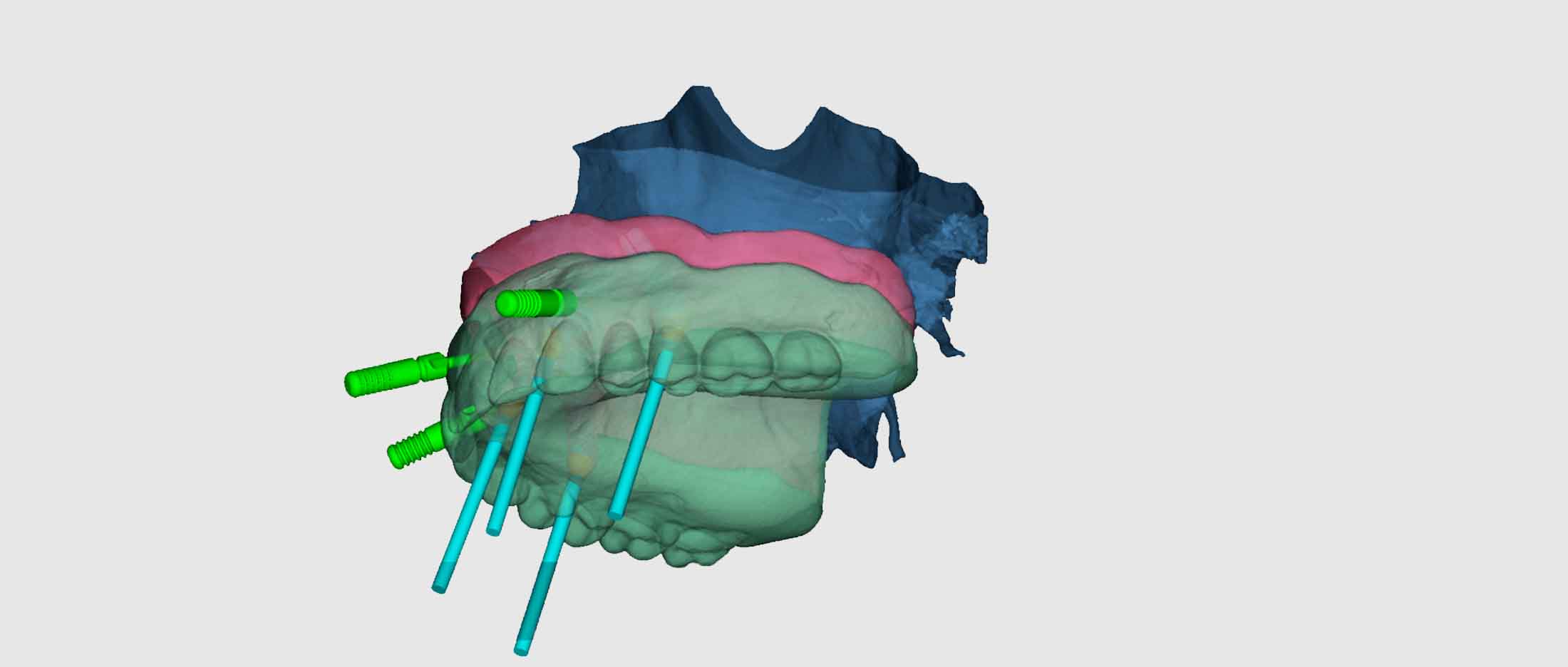
The beauty of IPS e.max Lithium Disilicate and the strength of Nobel Zirconia. The Zurick Bridge from Precision Elite is a unique combination of exceptional materials which brings patients a high strength, metal-free alternative to traditional dental prostheses.
Advantages of the Zurick Bridge:
Advantages of the Zurick Bridge:
- Exceptional esthetics
- Amazing strength for high durability
- Metal-free
- Perfect for implant cases
- Precision fit with CAD/CAM and Press technologies
Esthetic and Functional Harmony
The first priority of laboratory technology as it relates to cosmetic dentistry is proper function. Any cosmetic treatment plan needs proper occlusal records, lateral and protrusive movements, and correct maxilla-condyle relationships to help ensure long lasting results. This is critical as we employ laboratory techniques or systems of any kind. Indeed, esthetics minus function equals failure.
Dental porcelain systems have made quantum steps forward in an effort to mimic nature in color, form, and function. Chemists are continually creating stronger and more durable porcelains.
Materials such as silicon
nitride, quartz, alumina particles, and
lucite are being added to conventional ceramics.
In some all-ceramic systems, totally new
chemical structures are being introduced.
These include glass-ceramics, crys-
talline hydroxyapatite, tetrasilic, fluormica
(machinable ceramics), zirconia, and lucites.
One of the strongest materials is an infiltrated
glass. Perhaps the most interesting material
to date is a single-phase hydrothermal ceramic.
The advantages of an all-ceramic restoration compared to a ceramo-metal crown are many indeed. The transmission and dispersion of light through an all-ceramic bonded restoration imitates the "natural" appearance of translucency, vitality, and depth of color. This creates a better harmony with existing dentition that the discerning patient and doctor will appreciate.
The absence of metal substructures eliminates other problematic behavior such as:
- A "dark margin" appearance.
(although porcelain margins will help significantly) - Greying of thin translucent gingiva.
- An "opaque look" due to inadequate reduction.
- A monochromatic appearance.
Ducera, Inc., of South Plains, New Jersey, has introduced a
new category of ceramic. It is a single-phase,
hydrothermaldental ceramic called Low Fusing Ceramic, (LFC).
The manufacturer makes the following claims:
"The transmission
and dispersion of light through an
all-ceramic bonded restoration imitates
the "natural"
appearance of translucency, vitality, and
depth of color."
First, it is 47% stronger in flexural strength than metal ceramics. Due to an ion exchange surface layer inherent to this porcelain, it increases its strength in vitro. Other porcelains decrease in strength, especially at the ten to twelve year period as hydraulic pressure turns micro cracks into macro cracks that propagate under stresses such as thermal, load fatigue, or design.
In recent years, the all-ceramic restoration
has become the restoration of choice whenever
possible. This was primarily brought about
by the developments of resin luting cements
and dentin bonding agents.6 Coupled with
these are the before-mentioned reinforced
porcelain systems. The
success of the bonded restorations are well-documented
and studies do agree on the exceptional
effectiveness of this modality in both functional
and esthetic treatments.
Second, low firing temperatures allow a better, more stable, natural color format. The translucency is not clouded, opalescence is true to the ceramic and not a metallic oxide fritting.9 Light dispersion is very natural and similar to tooth structure.
Third, the homogenous and extremely dense nature of this ceramic material makes it easy to grind, and it polishes extremely well. This softer porcelain is unique in that all test results indicate it is "most like natural enamel" in functional wear properties.9 This creates a much less abrasive occlusal surface and enhances periodontal tissue health.
In our laboratory. Low Fusing Ceramic is utilized to encase ceramo-metal and all-ceramic restorations as per the manufacturer's recommendations. I have been very im pressed with the results of this new material. If the laboratory testing does extrapolate into every day clinical results, I perceive it to be the restoration of choice among the discerning dentists of tomorrow.
Although there are many porcelain systems on the market today, no system should be expected to be all-encompassing. Some systems function and/or appear different under certain circumstances."' Thus the integrity and talent of the ceramist-technologist will always be the critical factor in our pursuit of excellence.
Pursuant to this cooperative goal of naturally beautiful and functional smiles is good communication between the dental office and laboratory. Visual communications are perhaps the most convenient to use and best convey details and the expectations of the patient and doctor. Photographs, laboratory prescriptions, computer imaging, color mapping, study models, or videos are tools of necessity to obtain optimum clinical results.
The following cases incorporate the before mentioned materials along with some of these ideas.
This patient expressed a strong interest in remaking a poorly constructed porcelain to metal restoration on tooth #8, (non-vital) which had been completed just a few months prior. He also expressed a strong desire to close the diastema between #8 and #9, correct the rotated appearance of ft 7, and create a better overall color and contour harmony in the maxillary anterior region. At this point, photographs and study models were taken.
It was concluded that in order to reduce anterior stresses, slight coronal plasty w^ould be done on the mandibular lat erals and central and veneers would be made for teeth #7 and #9, along with the replacement of #8 with an all-ceramic restoration. This conservative approach proved to produce good results in restoring proper colors and contours.
An initial enamel reduction of 0.5 mm was
done using a LVS-1 Brasseler diamond bur.
The remaining facial bulk enamel was reduced.
Final preparations included a tape ing chamfer
that extended to the edge of the retracted
gingiva on each veneer. Tooth #9's preparation
did not
break the distal contact and a lingual margin
was established. Toward the mesial lingual,
the margin was again brought down to the
retracted gingiva to provide for the mesial
emergence profile. Tooth #7 was prepared
in much the same fashion; slightly more
reduction was made to the mesial facial
lobe for a more ideal contouring of the
veneer. Tooth #8 had previously been prepared
and only minor changes were made to "clean
up" the margins.
With the retraction cord in place on #7
and #9, the second cord on #8 was removed,
and a polyvinylsiloxane impression was taken
along with an
opposing arch. I was called to the office
to determine the shades to be utilized.
First, I wanted to closely match the adjacent
prepared teeth in color
and the degree of opacity exhibited bv ff7
and 9 at the same depth. A previously fabricated
shade tab was used, consisting of a 1:1:1
ratio of B-2, D-2, and D-3 opacious dentin,
and it was mixed with a 20% 1:1:1 ratio
of B-2, D- 2, and D-3 dentin." It was
determined that this should be used to build
up &8 and that a D-2 shade, plus a slight
ochergingival tone and an opal incisal halo
would blend in well.
Model and Die Work
Models and dies along with a soft tissue
model were prepared. The dies were trimmed
under a 10X stereo microscope. The dies
are painted with a removable varnish to
allow about 35
microns space for resin. All saw cuts were
then blocked out and an impres-
sion was made with Express STD (vinylpolysiloxan).
The refractory
material was then mixed, vibrated into place,
and allowed to set for 45 minutes. The cast
was then removed and trimmed that it might
be incorporated in an Accu-Trac tray with
additional refractory material and allowed
to dry. The tray and refractory are then
separated, sectioned, and trimmed to facili
tate the ease of handling and access to
the interproximal margins.
The dies are placed in the oven at about
400 degrees C to eliminate ammonia
from the refractory that otherwise would
severely contaminate the porcelain. The
margins are then marked and fired to place.
The "cure" bake
(stabilization and expansion) is performed
at 980 degrees C. The second
bake is that of a wash-bake nature at 925
degrees C to adhere the porcelain
into the micro porosities of the refractory
material itself; thus the porcelain
will not separate or pull away from the
die due to "porcelain creep" upon
vitrification. I believe these first two
firings are crucial for three reasons:
the tray, condensed, fired at 500 Degrees
C to 915 degrees C at a six
minute rise under vacuum, and then air fired
at 915 degrees C for 1 minute.
First, to insure intimate margin adaptation;
second, a well condensed and
homogenous internal surface; third, establish
basic color tones. Next, I set out the porcelain
palate. Remember, I want to build up #8
to mimic somewhat the prepared teeth #7
and #9. This was done and fired into place.
The corresponding shades were mixed to follow
the prescription. First a D-2 plus a slight
amount of ocher porcelain modifier was placed
on the cervical margins and a basic D-2
dentin build up was made along with the
D-2 +1 /4 B-l dentin that was also prescribed.
A vertical segmental layering was applied
with very little mammalon development. An
incisal 50 and 51 were used along with a
thin overlay of window, and opal incisal
was added to form a whitish halo effect.
Each was then removed fromthe tray, condensed,
fired at 500
Degrees C to 915 degrees C at a six minute
rise under vacuum, and then
air fired at 915 degrees C for 1 minute.
Contour and Glazing
The restorations were contoured to close
the diastema and correct the rotation on
#7. All surfaces were then layered with
LFC transparent and fired. Slight surface
texture was done with a med.-coarse diamond
point, and a final LFC glaze was done. The
contacts were checked, and the veneers and
all porcelain restorations were separated
from the refractory via Al
0 (25 micron) at 30 Ibs. psi.
They were each tried on the master dies and model. A slight contact adjustment and a slight margin overhang on the lingual of #8 was refined. All margins were checked for correct contours. Any adjustments at this point were done with a white rubber wheel and polished with diamond paste. Each was etched and silanated and delivered to the doctor for placement.
The patient's primary complaint and reason
for seeking treatment was that
#8 and #9 were too broad, and lighter in
value than her smaller-than-normal,
grey-appearing laterals. The yellow chroma
of the cuspids was stronger than any of
her remaining teeth. Isolated bleaching
was performed on #7 and #10 along with a
full lower bleaching treatment. At this
time a photo was taken for laboratory communication.
The teeth were prepared and another photo was taken to show the color and density of color along with other char acterization of the remaining tooth structure.
Polychromatic Layering of Porcelains
Porcelain placements consisted of a 1:4 mixture ofB-2 Opacous Dentin and B-2 Dentin, plus a touch of light yellow (to bump up the chroma and value slightly). The basic B-2 Dentin layer was verv thin and interspersed with a B-l lobe here and there. It was then brushed back from the labial incisal 1/3 of the build up. Then a vertical segmental incisal placement was done alternating a 1:2 ratio mix of window (clear), and [ncisal 50 (light blue-grey), with a 1:2 ratio mix of window (clear), and Incisal 51 (light grey), and a touch of T-5 (polar blue). Each build-up was removed. Enamel shaded contact areas were placed. The porcelain was condensed with vibration and moisture removal (tissue blot technique), then fired from 500 degrees C to 915 degrees C in 6 minutes vacuum with a 1 minute air fire at 915 degrees C.
Although this technique of multiple building and firing is more time consuming, it offers a system of checks and balances relative to the location of final crown contours, colors, and the appearance of enamel depth that looks natural.
Contour and Glazing
After firing the veneers, contacts were adjusted, final contours were established, and surface texture completed. The margins were also finished at this time.
An initial glaze was done with LFC glaze at which time a light opal halo was placed on each restoration and a few light to moderate decalcification (white) areas were added. Note: LFC stains are a fitted porcelain and metal oxide composition and not a metal oxide only. Thus they do not wear off or leach out as many conventional stains do over 4-7 years.9 When staining, a double glaze is a good idea with strong merit. A second LFC glaze was done, and the veneers are removed from the refractory via Al 0 (25 micron) and 30 Ibs. psi. Each was etched and silanated for delivery.
Conclusion
This new single-phase hydrotherrnal dental ceramic, coupled with sound techniques and polychromatic layering will create superior esthetic results. The physical properties and wear characteristics most closely match that of natural dentition of any tooth colored restorative available. You can ensure vour patients function and esthetics for years to come.


